On April 23, Dr Mary V Seeman died at the age of 89. She was a professor emerita at the University of Toronto and first Tapscott chair in schizophrenia studies at the University. In that role “she led research that revealed the biological mechanisms underlying anti-psychotic drugs, informing drug development and guiding treatment. Her research into gender differences in schizophrenia shaped treatment guidelines and opened new avenues for clinical research.”
She also established the first outpatient clinic for women affected by schizophrenia at the Centre for Addiction and mental Health. As the University of Toronto Psychiatry Department said in their obituary for her she was a pioneer in women’s mental health. In being awarded the Order of Canada in 2006, The Governor General noted “her lifelong dedication to improving the lives of Canadians living with mental disorders”.
Dr Seeman obtained her MD degree from McGill University in Montreal in 1960 and an honourary doctorate of science degree from the University of Toronto in 2002. She has authored 353 publications, served on the editorial boards of a number of psychiatric journals, was an inaugural member of the College of Reviewers on the Canadian Institutes of Health Research and an honourary director of Doctors Against Racism and Anti-Semitism.
Dr Seeman was originally born in Poland but had to flee her home with her family to escape Hitler but she and her family found refuge in Montreal. In 2021, she wrote about an event that occurred while she was a medical student at McGill. I’m mentioning it because of what is going on at universities throughout Canada and the US today – hatred towards Jews that many of us thought was from the past.
As a 3rd year student, Mary’s mother developed an acute gall bladder attack. She asked Mary to call the doctor who made house calls. Mary did not have his number but searched the phone directory for it and found what she thought was the doctor’s number. It turned out not to be her mom’s doc but another doc with the same name teaching at McGill medical school (and one of her own professors). This is what Dr Seeman wrote about that in 2021:
“He said, “I am not that snivelling Jew doctor. I don’t treat dogs and I don’t treat Jews.”
Those were the words. They’re imprinted in my memory. And that from a very well-known professor, the leader of our clinic group. The man I had to answer to the next day in the clinic.”
That was the late 1950’s and here we are in 2024 when Jewish university students are afraid to go to their classes. I thought we had evolved past that but I guess not.
In Dr Seeman’s passing, we have lost a giant helping to ease the burden of schizophrenia. Hopefully, others will contribute as much as she and her late husband, Phillip, did.
Here we go again. Another mental health week that talks in platitudes about having good mental health and does not mention severe mental illness and its impact on the sufferer and the sufferers family. I was planning to write about an article in the Journal of Psychiatry and Neuroscience that talked about how we ignore the serious for the worried well but then, I saw this very brave obituary in the Hamilton Spectator.
It needs to be read and I am posting it with permission of the family.
In April 2024, John died peacefully, in his home at the age of 76. John was the second child of Caesar (“Jake”) Cappelli, predeceased, and Maria (“Mary”) Cappelli. He will be missed by his siblings: sister Dea Cappelli Clark and younger brothers, Greg (Carolyn “Kegs”), Chris (Mary Elin), and Adam (Gail) and his nieces and nephews: Jason, James, and Alexandrea Clark, Stephen, Jake, Sydney and Lauren Cappelli.
Our tears are not for your death, dear brother, but for your life. John spent nearly 55 years battling schizophrenia. His life is the tragic narrative of the millions of loved ones suffering with mental illness, and must be told.
A promising, intelligent, trendsetter, mild-mannered, handsome, athlete and letterman from Cathedral High School, John graduated with degrees both in mathematics and physical education from McMaster University by the young age of 22. Immediately thereafter he began his teaching career at Delta High School. A year later his illness took him from the classroom.
In the years that followed his withdrawal from the classroom and society (in the early 1970s) John embarked on what became a perilous spiritual journey. Sitting in lotus posture, he would teach a small group of friends and peers his learnings of ancient philosophers and spiritual messengers. They listened raptly to his sincere and high-minded musings.
But like Icarus in Greek mythology, John may have soared too close to the sun. His hippie-era experimentation proved to be too alluring for his curious mind as he set out on what appeared to be a quest to find the greater meaning of life.
John’s subsequent and steady decline into extreme mental illness was very emotionally taxing on his parents and siblings as they searched tirelessly and unsuccessfully for answers and treatment. As the illness grew more and more acute with John refusing any medical treatment, he had many involuntary admissions to Hamilton Psychiatric Hospital. Episodes of physical assaults, coupled with his non-compliance to anti-psychotic medications led to family distancing. Nevertheless, familial love was constant and unconditional.
Pioneering family support for other parents and siblings dealing with this highly misunderstood illness, John’s parents and sister Dea together with a team of medical professionals at McMaster, founded Hamilton’s “Friends of Schizophrenics” in 1980, which subsequently amalgamated to become Ontario Friends of Schizophrenics.
There were court appearances and devastating newspaper articles publicizing some of the more embarrassing and delusional episodes caused by John’s illness. CBC’s documentary series Man Alive, profiled the first fifteen years of John’s painful journey with Schizophrenia, which included electric shock therapy. We could never appreciate just how ravaging this illness was for John at a time when mental health was massively misunderstood, and unsympathetically feared by most.
John suffered through many housing evictions, but unlike so many Schizophrenics, John was spared homelessness and roadside begging with the fortunate support of his family who were able to purchase a small home on the east mountain for him to live in alone in an environment that made him feel at peace.
The unwanted voices continued to haunt and taunt John prompting him to regularly dismantle the smoke detector, the heating and cooling thermostats, the TV antenna, his telephone and his overloading the electrical outlets. His many guitars, amps, turntables and VCRs and art (mainly mandala painting) were his companions.
He once asked his sister who was visiting him in hospital, “Do you suffer?” Her answer, “Not really. Do you?” His response “Every minute of every day.” Yet, he remained a man content in his own skin, harming no one, asking for very little, and wanting nothing more than life’s most simple offerings. Recently when greeted at the door of his home by his niece Sydney, she said “Hi John, do you know who I am?” He warmly responded, “No, but come on in!” John feared no one, judged no one, and trusted everyone. The only way to describe these last decades was that John was now dwelling in Purgatory.
Neighbours and his oft-visited pharmacist remarked that he was a lovely, quiet, and kind man. Compliance to some meds and family wellness checks brought about some reversal to his true personality. But elder age and mild dementia were starting to creep in. Where would we turn for his next level of care? John would no doubt refuse this transition, as he strongly disliked medical attention and living with others.
Not long into this latest dilemma, John’s poor nutrition, chain cigarette smoking, and his hermit-like existence caught up with him, leading to his inevitable release to Heaven. On a warm, sunny April day, John was found by his brother Adam who was doing a routine wellness check finally tucked in his bed for a sleep from which he would not awaken. He had now gone to that “other dimension” forever.
Cremation, followed by interment with his father, at Holy Sepulchre Cemetery will take place privately with his immediate family in June.
In lieu of a celebration of life in honour of John, the family encourages a donation to anyone you know who is struggling, or to a cause that is dedicated to the treatment, awareness and assistance to those suffering from mental illness. We are hopeful that honouring the solitary life of one man will awaken compassion, unconditional love and understanding for all afflicted brothers and sisters, daughters and sons, resulting in mental health awareness and activism now so long overdue.
If you knew John at some point in his life the family would be very grateful if you could share a story or a make a comment on John’s memorial page at www.Baygardens.ca
‘Now cracks a noble heart. Good night, sweet prince,
At the beginning of my journey into medicine and then psychiatry, I struggled, as all students of neurology, philosophy, and psychology do, with the concept of delusion, at least delusion as the product of mental illness.
What is the difference between a true belief, a lie, and a delusion? Or the difference between a harmless and shared religious delusion, and those religious delusions seen in bipolar and schizophrenia?
Well, I think I sorted it out for myself over the years, and became quite comfortable with the distinctions, while maybe getting it wrong a couple of notable times: my manic patient who asked for a weekend pass from the psychiatry ward so he could board a private plane they were sending to bring him to a conference in Salt Lake City. Clearly a delusion of grandeur? No. It turned out to be true.
And a Vietnam vet working in the kitchen of a bar downtown and who was sure the mob was trying to kill him, which I was pretty sure was a delusion, until the bar was firebombed.
A delusion is an explanation. It forms in the mind of a mentally ill person to explain an overwhelming feeling (mania or depression), or to quell an overwhelming fear, confusion, or explain an hallucinatory experience. It is singular, autistic, not shared by others. It can lead to behaviour that is destructive to self or others.
But a delusion can be developed, shared, nurtured, reinforced by others, in an otherwise healthy brain. This usually requires some degree of social isolation, isolation from conflicting explanations, along with membership in a cult with a charismatic leader.
The leader of a cult? Well, that’s a psychopathic liar who has found a way of living grandly, of maintaining power, control, wealth, and abundant sex.
Before the internet and social media these differences were clear. The conspiracy theorist, usually mentally ill, stood on a soap box in the town square, mostly ignored as he ranted, or he wrote letters to the editor, seldom published. The psychopathic cult leader could only grow his cult to a limited size, requiring communes and compounds and direct contact.
The cults became known when their compounds were raided, or they gathered to witness the end of the world, or to commit mass suicide, or when the actual purpose of the cult (always sexual exploitation) came to light.
I am thinking of this and writing of this because social media has changed the landscape. The delusional cult can now be virtual. You don’t have to leave home to join one. And now the messages of the cult can reach not just the disaffected, but also the mentally ill, the man living on his computer in his parents’ basement, a motel room, a boarding house, developing, or relapsing into, a mental illness.
With social media the delusions of a cult can infect increasing numbers of people, far and wide. And among those people the delusion reaches, are some who are mentally ill. And those with a mental illness, schizophrenia, depression, or mania, may singularly decide they are the chosen one, the chosen one to make a statement, to enact the logical end-game of the delusion, to enact revenge or violence, to commit mass murder, and die as destined.
Two recent examples are the man who immolated himself before the Trump trial, and the man who killed six women in Australia.
A school board allows a male teacher to come to class wearing outlandishly large prosthetic breasts with prominent nipples.
And now an Island Health Memo (BC) to acute care hospital staff instructs nurses not to stop open use of illicit drugs in hospital rooms, but, instead, to teach patients how to inject drugs into their IV lines, provide safe equipment such as crack pipes and burner kits, and instruct in the techniques of safe needle disposal.
Not to mention instructions to staff to teach “chest feeding” rather than “breast feeding” to new parents.
The first idiocy occurred under the guise of “inclusion, acceptance” of self-identity. The second idiocy apparently under the guise of harm reduction and decriminalization. The third apparently to be inclusive of …. of what biological apparition I am not sure. ?Presumably a trans person, biologically male, who has a chest rather than breasts, but still with sufficient mammary glands to produce milk? Or might it be a biological female who plans to have her/his breasts surgically removed once the child has outgrown “chest” feeding?
But back to the Island Health Memo.
I can picture how such a policy and memo might arise within a committee, a committee made up mostly of folks with aphantasia, or who simply lack the ability to imagine how a particular policy will play out with real people in real contexts.
“No. Wait. It’s okay. You don’t have to hide your stash, but let me show you how to inject directly into your IV line, rather than between your toes. Oh, and what is it you’re using by the way? The stuff you’re heating on a spoon with a cigarette lighter? You don’t have to tell me, really, but just in case it doesn’t mix well with your antibiotic drip, I mean is it fentanyl, oxy, heroin, crack, tranq. a mixture? Okay, I wonder how that will affect the anti-psychotic medication you’re receiving? Oh, never mind, let’s find out, shall we.”
But in all of these situations I think our very contemporary problem is finding a way to set sane limits, boundaries, codes, rules, without being exclusive, moralistic, and/or punitive.
When an addict is admitted to hospital for a psychiatric or medical condition the staff and doctors need to know what and how much and for how long he or she has been using, in order to anticipate and alleviate withdrawal symptoms. And to do this safely for all involved, using hospital-grade pharmaceuticals.
Not just allowing, but condoning and enabling, the use of street drugs in a hospital setting, is just plain nuts.
I await the million dollar law suit that will abruptly end this foolishness.
And, since writing this, the government has partly backed down.
Two recent papers outline the cause of homelessness and how it can be improved. The first is a report by Mr Justice Richard D Schneider that has been hidden in the bowels of the Government website since 2015. Schneider developed the Toronto Mental Health Courts. The second is a recent study just published in JAMA Psychiatry on homelessness out of the University of Calgary.
Justice Schneider looked at why we have seen such a huge increase in the mentally ill involved with the criminal justice system and points out how our changing laws have created that problem. The percentage of prisoners with mental illness has more than doubled between 1997 and 2008. Because of a weak Mental Health Act and the lack of sufficient psychiatric beds, those in need of help are either turned away or discharged before they are fully stable.
These unwell people often then end up committing some minor offence and land in the judicial system rather than taken to an ER. Once that happens, matters get worse. Any treatment is via the correctional system then, upon release, there is little treatment or opportunities and people find themselves with little to no employment prospects, they often begin drug taking for escape or self treatment and are lost.
Until 1978 when the Mental Health Act was changed, the act was based on the state holding a parens patriae role as a guardian of the ill. “Mentally disordered individuals are hospitalized if there appears to be a need to treat them and they are not availing themselves of the necessary treatment voluntarily.” This fell out of favour in large part thanks to the civil libertarians and the 1978 Act that replaced this became based on the concept of dangerousness. The state stepped in only if the person was a danger to himself or others. Declining health due to lack of help did not count.
As Justice Schneider said “we may only interfere with an individual’s freedom if he is perceived to be a danger to himself or others. If an individual is not seen as dangerous to himself or others he is free to roam the streets ‘madder than a hatter’. This latter model is the most common in North America.” Add to that the reduction on government spending on mental illness care so that there are even fewer treatment programs for people. The money that was saved from bed closures was to be reinvested in community treatment and supportive housing but governments neglected to do that.
The consequence of all this is that we have large portions of the mentally ill receiving little to no treatment or community support, ending up in and out of jail and filling the ranks of the homeless. If they are lucky, the parents do what they can but it is expensive and exhausting.
The recently published study out of Calgary looked at over 48,000 people from 19 countries who were homeless. Half were from Canada or the US. What they found was that 67% of them had a mental illness. Geographically, 77% of the homeless in North America had a mental illness compared to Australia (47%), Asia (59%), and Europe (60%). In fact, since 2010, the situation has been getting worse. Mental illness among the homeless has gone from 48% to 76%.
They suggested that “people with mental health disorders may be at increased risk of experiencing homelessness due to factors like housing affordability, limited access to care, low income, and problems reintegrating after receiving inpatient treatment.”
A 2023 study by the Fraser Institute found that Canada was near the bottom of OECD countries – 23 of 29 for psychiatric care beds per 1000 population, 18th on psychiatrists, on expenditures, we are 6th out of 8 countries on percent of GDP spent on mental health care at 7%. France and England were at 15 and 13%. The Canadian Alliance on Mental Illness and Mental Health put out a report card on services across Canada earlier this year and with a few exceptions it was F across the board on all measures. The best achieved by very few provinces was a D.
And so, what are we doing to resolve this horrific problem? Not much unless maybe you count kicking homeless out of parks or passing out syringes and Naloxone kits. No improvements in the law, increase in psychiatric and addiction treatment services, beds and programs. I may have missed it but I see very little advocacy if any from psychiatrists or medical professionals with suggestions for improving the situation. Same goes for our political leaders.
The New York City mayor is implementing increased involuntary treatment to try to improve the fate of the homeless mentally ill. Psychiatrists are demanding that more needs to be done. Their position is that after hospital care is essential along with community supports, assertive community treatment, supportive employment and housing first which involves wrap around support. And they say, lack of psychiatric beds is problematic.
California is implementing a Community Assist Recovery and Empowerment Act (CARE). This would provide increased housing, mental health and substance use services, and other essential services to help. They are investing $15.3 billion for homelessness and $11.6 billion for mental health programs to deal with the crisis. Of course, the American Civil Liberties Union (ACLU) and various disability groups are opposed. They believe that people should live in squalor and their delusions even if they lack the capacity (because of their illnesses) to realize they are sick.
What Dr David Laing Dawson suggests based on his experience watching the deterioration of the mental health system for the past 40 plus years is this:
Homelessness is a very complex problem with underlying factors of economics, available affordable housing, inflation, unemployment, education, family, addictions, addiction policies, municipal laws, provincial and state laws, increasingly incapacitating and lethal drug supply, and untreated mental illnesses.
In the meta study referenced above, it was estimated that substance use disorder contributed to the homelessness of 47%, and antisocial personality disorder 26%, while major depression accounted for 19%, schizophrenia 7% and bipolar disorder 8%.
Addictions (substance use disorders) and personality disorders are not easily treated. To make any kind of dent in this portion of the homelessness problem will require complicated changes to laws, affordable housing, specific programs developed, specialized support systems, rehabilitative activities, easily accessed medical care, and some form of persuasion…….
But if the above figures are accurate, and about 34% suffer from major depression, schizophrenia and bipolar disorder, this means 34% of homelessness is directly linked to treatable mental illnesses – illnesses we can successfully treat with prescription pharmacology, ensured compliance, combined with basic support and housing. And if the studies and estimates are accurate, that figure may actually be above 50%. And this means 50% of the homeless population are homeless principally because of untreated mental illnesses.
At some point people with these illnesses, usually, if not frequently, spend time in the emergency and psychiatric wards of hospitals. (see the Bryenton story)
So….
By law, mandate, or very strong policy, these hospitals could be ordered to never discharge a patient to the street. A place of residence and organized continuing care must be established before discharge.
Such a policy, strongly worded and monitored, would then force the hospitals to a.) involve families always, b.) liaise closely with social housing systems and social agencies, c.) use community treatment orders, d.) develop teams of professionals to manage the transition from hospital admission to life in the community with continuing treatment.
On April 9th, I watched on CBC’s Power and Politics the Minister of Mental Health and Addictions, Ya’ara Saks announce a 2024 Budget proposal of $500 million dollars for a Youth Mental Health Fund to help younger Canadians. Here is the Press Release:
Does this mental health fund include funding for “younger Canadians” who are experiencing their first psychotic break? Will it ensure access to a psychiatrist, and an adequate hospital stay and supportive housing upon discharge?
The Press Release reads “And, because many of them are still in school or just starting their careers, they are more likely to struggle with the costs of private mental health care”. Is the Minister not aware that we have Universal Health Care in Canada? Yes, psychologists need to come under Universal Health Care but we also need more psychiatrists who will treat serious mental illness.
The statement continues: “Through no fault of their own, Gen Z has inherited an expensive housing market, and a rising cost of living—both of which are causing unprecedented anxiety about their future. It is more important than ever that young Canadians get the support they need”.
Is the Minister aware that those with serious mental illnesses have faced a housing crisis since the beginning of de-institutionalization and that this crisis has been neglected for decades? The money that was to be saved from running the institutions was to go into appropriate community services like supportive housing but it did not. In fact, 77% of homeless people have a mental illness according to research just published on April 17/24
The statement continues: “The new Youth Mental Health Fund will help community health organizations provide more care for younger Canadians, and better equip these organizations to refer youth to other mental health services within their networks and partnerships”. Would it not make more sense to open up more hospital beds, so “young Canadians” who are experiencing their first psychotic break can receive the medical care that they need?
Instead many of those untreated “young Canadians” have entered the homeless population. I see them walking around talking to their voices on Yonge Street, sleeping in stairwells and begging for a plate of food at church breakfasts in the community where I live.
No-one cares.
The Press Release states that this money is to go to community mental health organizations. While there are some knowledgeable and empathetic community workers, most “Community mental health organizations” have a track record of not attending to the most seriously mentally ill adequately. Ask family caregivers of those who are seriously mentally ill who have had their complaints continually dismissed. I have spent years pursuing resolution to my concerns. This is how it appears to work: Complaints are forwarded to the executive director, who may either ignore them or offer a defensive excuse. Complaints are then forwarded to the Board of the organization who refer the complaint back to the Executive Director. Complaints are then forwarded to the local MPP who then forwards them to the Ministry which is usually followed by a message from the Ministry, some weeks later, that I need to express my concerns to the Executive Director.
Lack of Mental Illness Literacy.
According to The Honourable Marci Ien, Minister for Women and Gender Equality and Youth “The Youth Mental Health Fund is our commitment to making sure that their courage leads to the care they deserve. They’ve taken the first step; we’re making sure they’re supported for the next one.”
Does Minister Ien know that many with psychotic illness have the symptom of “anosognosia ” and are, therefore, not aware that they have an illness. So why would they reach out and make “the first step”? This lack of knowledge about serious mental illness among our leaders is unacceptable. It would seem that most mental health funding initiatives do not address the needs of the seriously mentally ill.
No Accountability.
Also included in this announcement is that the Federal Government will be “Providing $14.25 million in annual funding to the Mental Health Commission of Canada, to advance mental health in the priority areas of suicide prevention, mental health and substance use, engagement with Canadians, and population-based initiatives which includes children, youth, and emerging adults“.
In 2018, a report commissioned by Health Canada and conducted by Dr. Pierre-Gerlier Forest and Dr. Danielle Martin recommended that the Mental Health Commission of Canada be disbanded and can be found here.
Why were tax dollars spent on a federal review of the Mental Health Commission of Canada in 2018 which recommended that this organization be disbanded only to have funding continue for years including this latest bump in money?
How will Outcomes be evaluated?
The Press Release did not explain how the outcomes of the services provided by this money will be evaluated. According to the Press Release, the money is to go to improve the lives of “young Canadians” but what indicators will there be, to know that this outcome has been achieved?
This announcement of a Youth Mental Health Fund is another example of how our tax dollars are spent with no clear mandate, and no clear expectations set out. Families of those with serious mental illness have been witnessing this phenomena for years.
The Minister Needs to Explain:
If this money is also to go to help “young Canadians” with serious mental illness?
What is her knowledge of serious mental illness?
Is she aware of the devastating effects on those with serious mental illness and their families incurred by the policy of deinstitutionalization?
Does she see a connection of this poorly thought out policy and the current crisis in homelessness of many “young Canadians”?
Would not some of the money be better spent on opening up hospital beds and allowing “young Canadians” to get appropriate treatment for their emerging psychotic illness?
Given Ontario’s penchant for funding bureaucracies (e.g. The Centre of Excellence and the Establishment of a Mental Health and Addictions Ministry) rather than funding direct services, what guarantees do we have that this money will go towards youth in the Province of Ontario?
Both the Fraser Institute and the Canadian Alliance on Mental Illness and Mental Health gave negative reports on the state of mental health services this year. What components of these reports is this funding to address?
Recently the NIMH announced that in the U.S. the prevalence of schizophrenia and related psychotic disorders is between 0.25% and 0.64%.
This implies that our assumption of a 1% and higher risk (and prevalence) has been wrong, or that, miraculously, progress has been made in the USA in the prevention of schizophrenia. Unfortunately, this also implies that we need not spend as much money or attention on this serious illness.
But, of course, it turns out those figures arose from something called household surveys: phone calls to a representative sample of American Households. That 0.25% to 0.64% does not include the homeless, the transient, and the institutionalized. To be included one needs to belong to a household with a phone.
I suspect those figures actually represent only about half of the people in the USA suffering from schizophrenia, those who have phones and households, bringing us back to 1% or more when we include the others.
I was reminded of this by Bill Maher’s recent anti-woke diatribe on Canada. Officially, as he points out, Canada’s unemployment rate is 6.1 % vs the U.S. At 3.8%.
Well, it turns out Canada’s unemployment rate has never been as low as 3.8%. Rarely has it been under 5 percent.
It is easy to find how these stats are “calculated”. Google tells us that we get this number by dividing the number of unemployed people by the total number in the labor force, then multiplying by 100. It is much harder to find out how the number of unemployed and the number in the labor (or labour) force is determined.
In the USA it is, once again, a monthly survey of 2000 households. In Canada the numbers also come from a survey, though I became frustrated trying to find out how big and what kind of a survey.
Maybe our numbers of unemployed are almost double those of the USA. I doubt it. The fact we have never been as low as 3.8% would seem to point to a discrepancy in the calculations, the means of surveying, and the validity of the survey. Again, in the US, the survey is of households with telephones. It excludes the incarcerated, the homeless, and the transient.
Bill does make a good point about extreme liberalism provoking the rise of the extreme and dangerous right wing. But this essay is more a suggestion that when quoting any “statistics” in the press or media we should include the many caveats and limitations that come with such figures, and how they are actually derived.
This clever little book was published in 1989 and is still going strong. And I was reminded of it last night while watching commentary on the Israel Hamas Gaza war, and the overnight missile and drone attacks by Iran, as I listened to pundits, commentators, military historians, retired generals, and politicians weigh in.
All men of course.
And what struck me from their interpretations, conclusions, advice and prognostications, was that they too learned all they need to know in kindergarten, or perhaps between JK and grade 4.
But unlike the author of the original book who took to heart the words of his teachers, these men, as boys, received their instructions on the school ground, in the yard, at recess, lunch time, and after hours.
There were a few moments when the speakers looked at the complexities of large masses of people governed by a hierarchy, with many ambitious men sitting precariously at the top with the level below them coveting their power, but mostly these countries were discussed as if they were single, large, sentient beings obeying the boy-rules of the primary school playground.
A “few” years ago a boy in grade 4 was regularly bullying some of my grade 2 classmates and I was the tallest of the boys in my class that year. So it happened that I volunteered, or was chosen, (I don’t remember how it came about) to fight this grade 4 boy. At recess a crowd gathered, creating a circle, a ring, and in that ring this boy and I squared off. I’m sure we tugged and pulled and pushed for a bit and then I got him down on the ground, with me on top, in control. But with a free hand he grabbed me by the throat and squeezed. I got off him and stood up. He left with his friends and never bothered my classmates again, and I was briefly a hero, though in reality I quit because he was choking me. And that was the first and last physical fight of my life, so far.
But at age 7 I was obeying the rules of human conduct espoused last night by those pundits on my television. And it did work in the school yard. The bully went away.
But surely to deescalate this situation in the mid east and move in the direction of a lasting peace we need to go beyond the wisdom and understanding of a 7 year old.
The decision makers in Iran, mindful of the ambitious cadre below them, responded as if in the school yard, tit for tat. But they know of Israel’s iron dome, it’s sophisticated systems. So they put on a show, a multimillion dollar barrage of missiles and drones, that would and did cause very little damage.
Leave it be. Israel and the US need not respond. The leaders of Iran don’t want to turn the mid east into an inferno. It was puffery, showing off, maintaining their politics.
Now it is Netanyahu’s time to be an adult, to leave behind the retaliation of the school yard, and work with whatever sane, adult world leaders he can find, to end this war.
Over the past few months, we’ve done a number of blogs on the problems of supportive housing using a Christian charity (Indwell) as the example and published some research on how it operates by Karen Allin in Mississauga. Karen has no personal involvement with serious mental illness but she was concerned when Indwell wanted to build near her. She found my blogs and that concerned her about their competence. At the public meeting she attended, some of Indwell’s own residents came and complained about the failures of that organization.
And then I heard from another resident at Indwell in a building in Hamilton with complaints from that place. She and Karen conducted their own survey of residents and the results were not pretty. Karen’s report with those results I published last week.
Thus far, no one in any position of authority has shown any interest in looking into this situation despite Indwell getting about $123 million in financing from all levels of government and I’m not the least bit surprised. What impressed me about Ms Allin’s original report on Indwell is this statement: “Imagine the joy a potential tenant feels when they are told there is space for them in an affordable, supportive, housing apartment. As highlighted in this report, that joy quickly turns to a nightmare for many “
It turned out to be a nightmare for my wife and I when our son got a place at Indwell. We initially expected that he would have a nice place to live where, if problems arose, they would be taken care of. Problems continually arose involving violence (one murder), assaults, drug trafficking, to name a few that were never resolved.
What is happening at Indwell is not unique. There are no enforceable standards or oversight from government on how the tenants are cared for or how the grants are administered. As one comment on the last post on this topic said “All organizations that house individuals with mental health problems, etc. need to be held accountable, with transparent reports, financial statements, tenant feedback, etc.”
That is not generally done because those with serious mental illness are the “ass end” of our healthcare system. Nobody in authority seems to care which is why we have the mess on our streets that we do. As statistics have shown, a considerable majority of those living on the streets have untreated mental illnesses. We do hospitalize people for as short a period as possible and then kick them out to the street with little or no follow up, no living arrangements and little money. They either fend for themselves or the families help to the extent they can.
It wasn’t always like this.
My blogging partner, Dr Dawson, commented in a recent e-mail to me that from his experiences as psychiatrist in chief at the Hamilton Psychiatric Hospital “We were doing the right stuff in 1975 : family involved always, had one team member assigned to each community agency to maintain communication and resolve problems. Prioritized the seriously mentally ill. 1985 started special team to help transition from hospital to community. I think I always naively assumed progress would continue.” This is a longer review of how much we’ve deteriorated from the 1980’s to today
And what it takes to get proper medical care for a child with a serious mental illness was outlined recently in this blog by Dr Richard O’Reilly In that blog, Dr O’Reilly was discussing what it took Marlene Bryenton of PEI to rescue her ill son from the streets of Toronto. He said “families are often exhausted due to the effort needed to look after someone with a severe mental illness: particularly the effort sometimes required to ensure that a loved one stays on treatment. Family caregivers repeatedly tell me that they feel shunned and defeated by the system.”
He added, “The story of Andrew Bryenton demonstrates what I have always believed – that the mental health system will not meet its duty to provide appropriate care and treatment to people with severe mental illness until family caregivers come together and force it to do so.” The problem is that family caregivers are too exhausted to do that.
I’m fortunate that I live in a city that has a psychiatric hospital and even has a dedicated psychiatric ER but it takes all of our energy to ensure adherence to good medical practices. The senior bureaucrats know me well. There was one time when our son needed to be seen by the ER so I took him. That is not as simple as it sounds for the local psych ER is (or was) out of a 1950’s film, the Snake Pit. At one point, it was so bad that the medical school pulled all its resident docs out of there because of violence. I’m told it is now much better.
In order to get emergency psychiatric care, the patient first has to be cleared medically. The reason for that is a man with schizophrenia had pneumonia and his family doc sent him to the ER and called ahead. But, the ER staff knew him to have schizophrenia so made him wait for psychiatry even though he told them he was physically ill and had been sent there by his family doc. When he couldn’t breathe, he was given a paper bag to breath into as they assumed he was having a panic attack.
He arrested and died on the waiting room floor.
Now, all psych patients must be cleared medically which is sensible but then you have to convince the ER doc you want psychiatry. So, I take my son in and he gets checked by medical, they find no problem and try to discharge him. I then had to get into a shouting match with the doc so that he would be referred and we waited. No one came and they called psych again and again.
Finally, I could not wait any longer and told them I was leaving and ensured that they were aware my son was waiting for psych. Next morning, I called ER psych and they had never heard of him and refused to tell me where he might be (confidentiality you know). The switchboard told me he was still in the medical ER. Fortunately, I knew the VP of mental health services and her secretary arranged a search party and my son was found on a chair in the hall of the ER. He sat there in a psychotic state all night and no one noticed or asked why he was there.
My mention of lawyers at a meeting with hospital bureaucrats gets a lot of apologies but why did I have to even do that?
That wasn’t the first time I went head to head with them and it wasn’t the last but it leaves you exhausted. If families don’t do that, our adult kids suffer but when we do, it wears us down.
Imagine if you had a family member with cancer or some other serious and/or chronic condition and you had to do that as well. They don’t have to do that and we shouldn’t have to do that either. These are illnesses not moral failures and there are good treatments and supports but we mostly don’t get good treatment or good supports.
And God knows that we all want to take back our streets and parks from all the homeless who congregate there. Our society let this happen and society can correct it if only we properly fund treatment, rehabilitation, proper supportive housing, meaningful activities for people. Most European countries can do that. Instead, we literally piss away funds to groups like Indwell and all the other similar places to do what?
As someone in BC commented on last weeks blog,” I blame the government. Here in B.C., we used to have many properly staffed, licensed care facilities. Then the Provincial government decided to pass the Assisted Living Act, which allowed for the privatization of care facilities that would no longer require regular supervision to operate. All political parties were united in agreeing to this fiasco, so all are equally guilty of the disastrous housing shortage that ensued for many poor people — especially the mentally ill & the elderly who require regular, ongoing properly supervised care and other supports to live safely & with dignity in the community.
If anyone wants to see what is called here “the show’,” come to Vancouver & take a stroll by Hastings & Main. It is truly heartbreaking”
Just last week, the associate minister of mental health, Ya’a ra Saks, a yoga teacher among other qualifications, announced $500 million to youth mental health – not illness but health. The press release stated that: “It is critical that youth have what they need to build a happy, healthy start in their adulthood. Mental health care is an essential part of ensuring every young Canadians can reach their full potential, and that helps Canada’s economy reach its full potential, too.”
So what are they going to do to make youth happy? They don’t say but what will make many people happy is if we provide the resources to help those with serious mental illness. Stay tuned for more on this latest effort in uselessness from our government. .
The Housing First model is based on the theory that if homelessness is caused by a lack of housing, then provide people with immediate access to affordable, supportive housing. Supports need to address: mental and physical health, substance abuse, education, employment and general life skills.
Critical Characteristics of Supported Housing and Seeking Supportive Housing are two Canadian reports that provide more detail about the range of supports that residents are looking for. Some of the many supports mentioned in the reports include: 1) Support with independent living, such as cooking, cleaning, managing finances, and 2) Support in preventing and managing a crisis, such as developing relationships, anger control, avoiding unsafe situations, and coping after a crisis.
In theory, supportive housing sounds fantastic.
Indwell is a Christian charity providing affordable supportive housing. They have 27 buildings, with 9 more in the pre-development or development stages. Indwell houses over 1200 tenants.
In December 2023, Indwell held a public meeting after they purchased a vacant lot in Mississauga. At this meeting we heard from Indwell tenants saying they do not feel safe living at Indwell. Because of this meeting, I decided to do more research on Indwell and produced a report “A Look Inside Indwell”. In February, I wrote a guest blog: When Supportive Housing Becomes a Nightmare for Vulnerable Tenants.
After that meeting, my city councillor formed a working group with Indwell and some local residents. Although Indwell says they provide wrap-around supports, at this meeting Indwell said the main support they provide is affordability. If that is the case, then why does Indwell say they provide supportive housing? When asked about safety concerns, the response from Indwell was that it was just a few disgruntled tenants and that we did not hear from the many tenants who are happy living at Indwell.
In March, I created a survey for Indwell tenants. Another Indwell tenant from Hamilton helped to survey 46 tenants representing about 80% of her building. Here are some of the results.
At a Region of Peel Council meeting in February, Jeff Neven, the CEO of Indwell, told the councillors that Indwell is safe; safety is their utmost concern. Yet, 31 out of 46 Indwell residents, or 67% of the respondents said that they sometimes, rarely or never feel safe living at Indwell. Is this really just a few disgruntled tenants? Is the Christian charity lying about providing safe housing? Or, are the tenants lying about how safe they feel? The tenants have no reason to lie.
One tenant described that another tenant repeatedly threatened to kill her. She said she started using a buddy system when she had to leave her apartment. She informed Indwell staff about the threats and Indwell told her that he said he never threatened her. Indwell stated, “My advice when there’s conflicting information is to always take things with a grain of salt”. After he threatened her again, the response from Indwell was, “Your safety is important to us. … Because of confidentiality, I am unable to share what action we’ve taken as landlords to uphold this responsibility.”
The resident then went to see the Crown Attorney with the complaints. The Crown took action when Indwell did not and, as a result, the man plead guilty to three charges: 1) July 31, 2022 – Utter threat to cause death, 2), Oct. 4, 2022 – Failure to Comply with undertaking, and 3) Oct. 30, 2022 – Utter threat to cause bodily harm.
For over 3 months, this tenant did not feel safe in her apartment because of another tenant threatening to kill her. She said that during this time, she did not receive any support from Indwell. Yet Indwell says they provide wrap-around supports. Indwell says they stay with their tenants in difficult situations and they adjust the support accordingly. Again, do you believe the tenant or do you believe Indwell?
Furthermore, 21 of the 46 respondents stated they have been verbally or physically assaulted by another Indwell tenant. That is not acceptable. It does not appear that Indwell provides supports relating to anger management.
So what types of support does Indwell provide? At the Region of Peel meeting in February, Jeff Neven said that Indwell connects tenants with a doctor and helps tenants get ODSP. He also described if a tenant gets a new dog and that dog is a real barker, then staff help to remedy the situation. Is a barking dog the best example that he could think of? Or, is it a true example of the extent of support that Indwell provides?
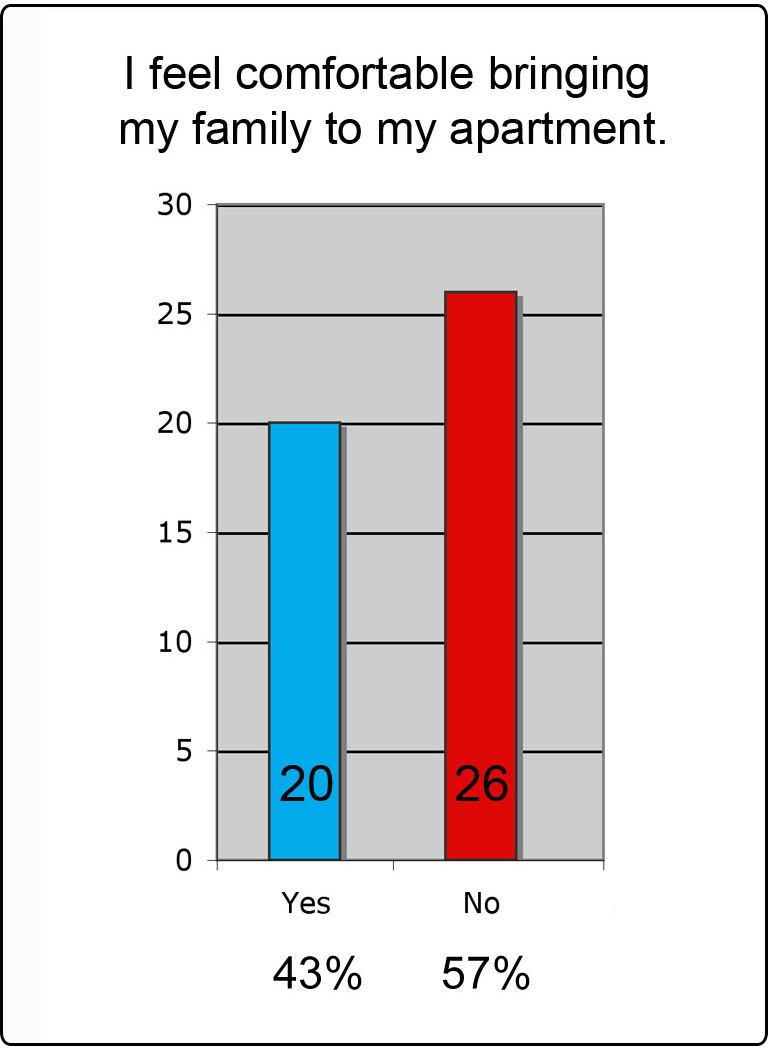
Of the 46 survey respondents, 26 respondents, 57%, do not feel comfortable bringing their family to their apartment. Likewise, 26 tenants said they would not recommend Indwell to a friend. Along with the verbal and physical threats, tenants in this building have seen overdoses, deaths due to overdoses and even a murder. On Jan. 7, 2024, CHCH reported one Indwell tenant violently assaulted another tenant. Other residents are saying this was a drug deal gone bad. The man who was assaulted was left crippled, with brain injuries and he died shortly afterwards. This murder was the second at an Indwell building in Hamilton. According to the Hamilton Spectator “Hamilton’s Parkdale Landing was to provide safer supportive housing — but then a murder happened”.
The tenants shared their frustrations with how the buildings are managed. One tenant complained about finding feces in the washers and dryers. Additionally, there are many complaints about apartment unit takeovers, trespassers sleeping in stairwells, prostitution, and tenants doing and selling drugs in the building.
How is any of this supportive?
In the last couple of years, Indwell has received over $123 million in funding and forgivable loans from federal, provincial, municipal governments and Canada Mortgage and Housing (CMHC). Will someone in government hold Indwell accountable, suspend future funding for Indwell and do a full due diligence on Indwell, including if Indwell provides safe and supportive housing?
Before writing this blog, I asked Jeff Neven from Indwell for an interview. I even gave him the titles of potential articles, including: 1) A Christian Charity so Focused on the Heavens that They Cannot See the Violence in Their Buildings, 2) The Many Hypocrisies of Supportive Housing, 3) The Failures of a Housing First Model, 4) When Supportive Housing Creates More Problems than Supports, and 5) Christian Charity Begs for Forgiveness, After Years of Lying about Providing Safe Housing.
Teresa Howe, the Community Engagement Manager from Indwell responded:
“For 50 years we’ve been providing supportive housing that transforms lives. Each new door that we open is done together with many partners; each new home is a solution to homelessness. The safety and security of each tenant is important to us and we continue to work with both our tenants and partners to ensure safety and address concerns.”
What will it take for Indwell to see the light and realize that they are failing to provide safe and supportive housing? Mr. Neven, if you are reading this, I would still like to write the article “Christian Charity Begs for Forgiveness, After Years of Lying about Providing Safe Housing”.