Karen Allin
The Housing First model is based on the theory that if homelessness is caused by a lack of housing, then provide people with immediate access to affordable, supportive housing. Supports need to address: mental and physical health, substance abuse, education, employment and general life skills.
Critical Characteristics of Supported Housing and Seeking Supportive Housing are two Canadian reports that provide more detail about the range of supports that residents are looking for. Some of the many supports mentioned in the reports include: 1) Support with independent living, such as cooking, cleaning, managing finances, and 2) Support in preventing and managing a crisis, such as developing relationships, anger control, avoiding unsafe situations, and coping after a crisis.
In theory, supportive housing sounds fantastic.
Indwell is a Christian charity providing affordable supportive housing. They have 27 buildings, with 9 more in the pre-development or development stages. Indwell houses over 1200 tenants.
In December 2023, Indwell held a public meeting after they purchased a vacant lot in Mississauga. At this meeting we heard from Indwell tenants saying they do not feel safe living at Indwell. Because of this meeting, I decided to do more research on Indwell and produced a report “A Look Inside Indwell”. In February, I wrote a guest blog: When Supportive Housing Becomes a Nightmare for Vulnerable Tenants.
After that meeting, my city councillor formed a working group with Indwell and some local residents. Although Indwell says they provide wrap-around supports, at this meeting Indwell said the main support they provide is affordability. If that is the case, then why does Indwell say they provide supportive housing? When asked about safety concerns, the response from Indwell was that it was just a few disgruntled tenants and that we did not hear from the many tenants who are happy living at Indwell.
In March, I created a survey for Indwell tenants. Another Indwell tenant from Hamilton helped to survey 46 tenants representing about 80% of her building. Here are some of the results.

At a Region of Peel Council meeting in February, Jeff Neven, the CEO of Indwell, told the councillors that Indwell is safe; safety is their utmost concern. Yet, 31 out of 46 Indwell residents, or 67% of the respondents said that they sometimes, rarely or never feel safe living at Indwell. Is this really just a few disgruntled tenants? Is the Christian charity lying about providing safe housing? Or, are the tenants lying about how safe they feel? The tenants have no reason to lie.
One tenant described that another tenant repeatedly threatened to kill her. She said she started using a buddy system when she had to leave her apartment. She informed Indwell staff about the threats and Indwell told her that he said he never threatened her. Indwell stated, “My advice when there’s conflicting information is to always take things with a grain of salt”. After he threatened her again, the response from Indwell was, “Your safety is important to us. … Because of confidentiality, I am unable to share what action we’ve taken as landlords to uphold this responsibility.”
The resident then went to see the Crown Attorney with the complaints. The Crown took action when Indwell did not and, as a result, the man plead guilty to three charges: 1) July 31, 2022 – Utter threat to cause death, 2), Oct. 4, 2022 – Failure to Comply with undertaking, and 3) Oct. 30, 2022 – Utter threat to cause bodily harm.
For over 3 months, this tenant did not feel safe in her apartment because of another tenant threatening to kill her. She said that during this time, she did not receive any support from Indwell. Yet Indwell says they provide wrap-around supports. Indwell says they stay with their tenants in difficult situations and they adjust the support accordingly. Again, do you believe the tenant or do you believe Indwell?
Furthermore, 21 of the 46 respondents stated they have been verbally or physically assaulted by another Indwell tenant. That is not acceptable. It does not appear that Indwell provides supports relating to anger management.

So what types of support does Indwell provide? At the Region of Peel meeting in February, Jeff Neven said that Indwell connects tenants with a doctor and helps tenants get ODSP. He also described if a tenant gets a new dog and that dog is a real barker, then staff help to remedy the situation. Is a barking dog the best example that he could think of? Or, is it a true example of the extent of support that Indwell provides?
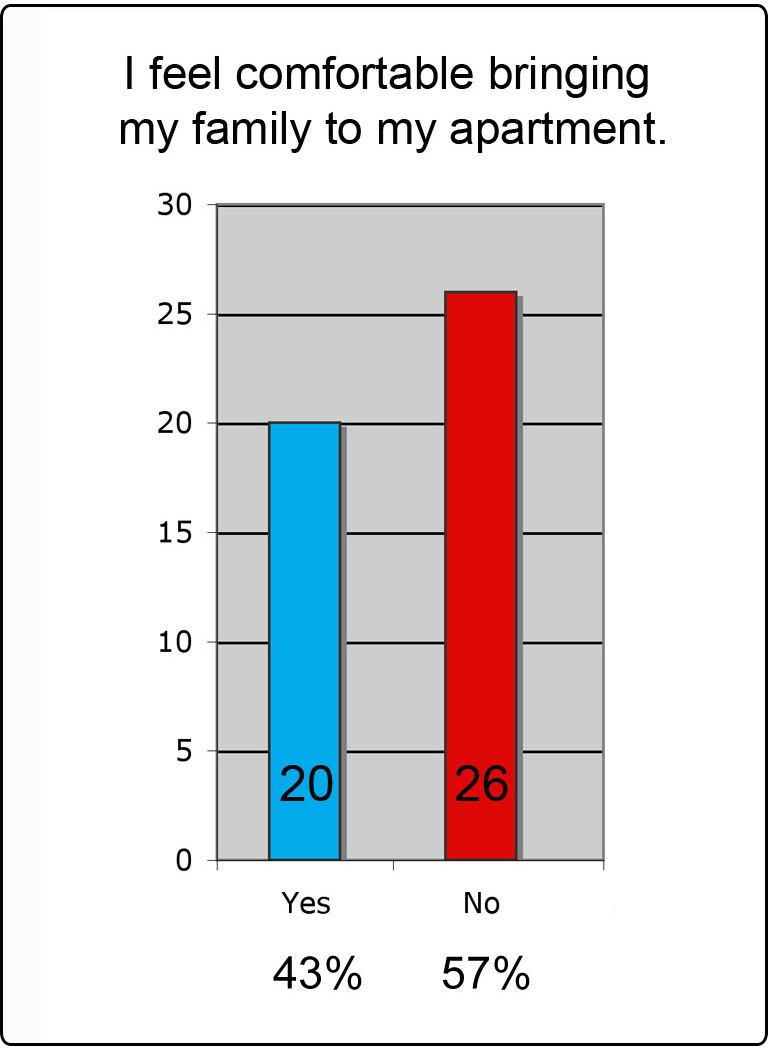
Of the 46 survey respondents, 26 respondents, 57%, do not feel comfortable bringing their family to their apartment. Likewise, 26 tenants said they would not recommend Indwell to a friend. Along with the verbal and physical threats, tenants in this building have seen overdoses, deaths due to overdoses and even a murder. On Jan. 7, 2024, CHCH reported one Indwell tenant violently assaulted another tenant. Other residents are saying this was a drug deal gone bad. The man who was assaulted was left crippled, with brain injuries and he died shortly afterwards. This murder was the second at an Indwell building in Hamilton. According to the Hamilton Spectator “Hamilton’s Parkdale Landing was to provide safer supportive housing — but then a murder happened”.
The tenants shared their frustrations with how the buildings are managed. One tenant complained about finding feces in the washers and dryers. Additionally, there are many complaints about apartment unit takeovers, trespassers sleeping in stairwells, prostitution, and tenants doing and selling drugs in the building.
How is any of this supportive?
In the last couple of years, Indwell has received over $123 million in funding and forgivable loans from federal, provincial, municipal governments and Canada Mortgage and Housing (CMHC). Will someone in government hold Indwell accountable, suspend future funding for Indwell and do a full due diligence on Indwell, including if Indwell provides safe and supportive housing?
Before writing this blog, I asked Jeff Neven from Indwell for an interview. I even gave him the titles of potential articles, including: 1) A Christian Charity so Focused on the Heavens that They Cannot See the Violence in Their Buildings, 2) The Many Hypocrisies of Supportive Housing, 3) The Failures of a Housing First Model, 4) When Supportive Housing Creates More Problems than Supports, and 5) Christian Charity Begs for Forgiveness, After Years of Lying about Providing Safe Housing.
Teresa Howe, the Community Engagement Manager from Indwell responded:
“For 50 years we’ve been providing supportive housing that transforms lives. Each new door that we open is done together with many partners; each new home is a solution to homelessness. The safety and security of each tenant is important to us and we continue to work with both our tenants and partners to ensure safety and address concerns.”
What will it take for Indwell to see the light and realize that they are failing to provide safe and supportive housing? Mr. Neven, if you are reading this, I would still like to write the article “Christian Charity Begs for Forgiveness, After Years of Lying about Providing Safe Housing”.

This article addresses the problems with “supportive housing” with a good dose of reality. Alas, this seems to be the dilemma with all housing of vulnerable people, including nursing homes. Throwing valuable taxpayer money into these projects is the easier part. Delivering responsible and viable living quarters is the real challenge. Mental illness, addiction, old age physical and mental problems, are always messy and hard to deal with. They are not pretty to see, and the public in general would just like to see the government handle the problems without much fanfare.
All organizations that house individuals with mental health problems, etc. need to be held accountable, with transparent reports, financial statements, tenant feedback, etc. In particular, the public statements they make in reference to success stories, activities and positive outcomes (in brochures, for example)need to be scrutinized carefully.
In a perfect world, there would be proper government surveillance and integrity in the hierarchy of these organizations. In reality, this does not exist to any great extent , even if there are some good individuals and politicians out there.
So, I applaud this blog in its effort to expose some serious gaps and misconceptions. The problem with funding is black and white and easier to tackle. The human side, unfortunately, is not.
LikeLiked by 3 people
Thank you Maria for your insightful comments. Sadly we see money awarded by funders who unfortunately do not follow up on where the money has gone. The money should be going to robust individualized programming that ensures that the tenant is meaningfully engaged, that medication is monitored, and that there be regular visits to health care professionals. There needs to be transparency. When there are genuine concerns about safety, these concerns should not be diminished but taken seriously. Standards for care need to be developed and followed up on with regular on sight visits.
LikeLiked by 3 people
Katheleen, RIGHT on! YOURS in a nutshell. Oversight, continuous audits, guidelines, regular robust surveillance that keeps things on track (feet to fire for promises proffered).
LikeLiked by 2 people
To quote David Ross, a tenant at Indwell, “Lumping addiction and mental illness
together is stupid. It just doesn’t work.” I agree with David.
In Kingston we have the sad saga of the HUB. Clearly the camp site Belle Park( public park) …. next to the HUB is facing off with the Court order to not camp during the day. Pack up and move on during the day is the dilemma. VERY hard to enforce!Just google the articles in the Whig Standard and on Global News and the mess is evident. The hub has a safe injection site apparently ?
The obvious problem which was long in the making has now come into focus ! Drug addicts are living in the same proximity with those with serious and persistent psychotic illnesses. And the drug dealers are circling the place . There is no doubt that this a recipe for disaster. Neighbours near the site are terrified by much of what is going on. Fires on the site require many visits by the Fire Department. Neighbours have to cope with people shooting up on their porches etc;
A group of eight or nine doctors sent a letter to oppose the city attempting to clear the site during daylight hours. Now the civil libertarians have got into the issue. Interestingly enough one former addict (8 years clean) has stated in a long article in the whig standard that it was forced hospitalization that started him on the journey of recovery. He now runs his own business. With forced hospitalization came social supports and a way forward.
I would hope that the doctors who co signed the letter did more on the realistic side to go to the route of the problem. Serious untreated mental illness. 2, be realistic about addicts. 3. Push for a more useful Mental Health Act and more mental health beds
Compassion through understanding would go a long way to steer in the right direction. Presently all attempts to solve the mess are just pushing the dangerous chaos down the road. It is chaos now and this will only get worse.
LikeLiked by 3 people
Post script. I am reading Marilynann Baker’s pain inducing blog. I quote her ….
“Ah, but so what? The anti-psychiatry zealots insist that we stop “medicalizing” people whose behaviours are merely eccentric. Quaint. Outside the norm. They just are living life as they wish, and we don’t have the right to interfere. We, the worried family and friends, shouldn’t judge them by our own standards of how one should live a life. ”
Those that treat this illness as though it is lifestyle choice make me want to scream and sue those who peddle and benefit by such views. BUT they have control; of the system unfortunately. What is more some so called professionals are aiding and abetting the current state of affairs, by not speaking out.
Shame on the Mental Health Commission of Canada for doing nothing about coming up with meaningful proposals to mend the system of care for the serious and persistently mentally ill They squandered a lot of money !
Someone with energy youth and courage needs to step into the breach and take up the challenge once again for medical care and justice for those who are trapped in psychoses for want of treatment. The tragedy is that in this era we have treatments that often work, but they are not used because of the anti treatment brigade. many of them are con artists.
LikeLiked by 1 person
Yes, yes, re supported living, “the theory is fantastic”! Your example, city Hamilton’s Indwell (charity for affordable supportive(sic) housing), is or was similar to Vancouver’s Brightside (and its predecessor). Brightside runs Glynn Manor public housing, bachelor suites–oversight (by and of Brightside, the funded, resourced, agency) didn’t undertake a role as long-term support for ongoing mental health issues and they didn’t tell anybody that they didn’t. The two seem similar or are the same.
Inquiry starting 2020 hasn’t resulted in acknowledgement that inpatient and long-term care or treatment has been updated by understanding or with improvements. I started out with a sense deaths were limited to 2018-19. Unmonitored isolation, maybe dropped-threads by personnel at Outpatient Clinic East Hastings, patients sent home from perhaps tumultuous inpatient treatment with symptoms including being frightening of physical recovery, that possibly predicted preventable deaths in Glynn Manor.
We are left to understand deaths after treatment and without supports is normal; victim blaming as though patients decided for themselves to be ill, illness as a choice. Strange is that health professionals seem to view patients as alone and view a person’s long-term supporters as an issue. I figure this amounts to, “I wasn’t there so it didn’t happen,” which seems a typical hole professionals can fall into, where context of outside 4-walls of exam room are lost on them.
Health professionals can have blinders about “who” a person is, including being wary or dismissive of a patient’s long-term supporters, waving-away the idea anyone but them understands help for a patient’s pain. A medical person asks a patient to explain why they feel distressed, as if illness were a choice–and possibly find themselves, together, seeking meaningful personal relics from life, extrapolating that, You can be less that way, guided by how I see things, a personal template that works for me. A sunny hopeful resolution, try your best.
My sense is that scrutiny or investigations are secret and confidential–as if to help or protect patients. One effect is it saves paid personnel embarrassment or from self-searching, including changing protocols and behaviors that OTHERS would benefit from, if only they knew.
Newbies, naive, confident, are blind of insights when they find themselves in the same circumstances–erring on the side of trusting a suffering person to somehow KNOW when to cave to care instead of caving to internal demands of their illness! Not telling anybody–though practices by individuals that were involved who subsequently developed better insight into nature and symptoms of mental illness and recovery, particularly eating disorders–doesn’t doesn’t promote better practices. Status quo, is blithely trusting people’s fate to known natural course of illness, because of arbitrary absence of contact or connection, where former patients (experiencing incapacity) have the impossible task of finding-it-in-themselves to know how to reach out when they couldn’t, a symptom.
Solutions are complex–and one insight is the not-subtle difference between “disability” and “illness.” Your, Opinion author Karen Allin’s, 1. “INDEPENDENT living, cooking, cleaning, managing finances; and 2. “SUPPORT in preventing and managing a crisis, e.g., fraught relationships, anger control, unsafe situations, coping after a perceived crisis.” As if “independence and support” are similar and as if an alteration of abode is a fix that takes care of both.
Like Dr. Philpott said on CBC today, April 9, 2024, you can’t dump a pot of money on health professionals and expect “a system” to grow from a vacuum of interest (where understandably there is self-interest).
Yes, “wrap-around” supports as the myth! Prior to Sep 2018, Vancouver, there was an agency, COPP, Community Outreach Partnership Program, (a single social worker person at least), that made a difference by continuous routine unrelenting skilled informed contact with former hospital patients with mental health issues (eating disorders anyway), that amounted to face-to-face meetings at a cafe, that meant reflecting together on current status, and that might indicate required guidance for doing hard things, including applying for care and treatment for recovery of irrational thoughts, behaviors, at least partly based on physical starvation status–to guide a person back to inpatient for familiar rigid routines to top-up recovery, if confusion or distress, an episode, overtook their ability to cope. A face-to-face cup of tea that results in a compassionate pronouncement, “You, have had enough,” and presenting a thorough plan, required to get back into recovery, available but frightening for a person that cannot betray their illness for the perception of pain represented by undertaking recovery.
The Community Outreach Partnership Program, COPP, suddenly went unfunded, maybe due to perception of duplication of services–outpatient clinic “can do that,” without remembering to spell-it-out to personnel, what that role might be like! And forgetting that twice is better than none-se, that “It is ALWAYS better to be redundant than remiss”–my sense is that authorities felt there was overlap so a cost-savings, because possible personnel of the Outpatient Clinic for Mental Health, East Hastings, a social worker or counselling available, might intuit a role for themself–for which a former patient had to inquire. But, “Out of sight, out of mind,” an eating disorder sufferer is afraid of betraying their illness, and has perception of dread and pain from the process of recovery. An eating disorder sufferer feels their behavior is in their control–though they an episode means they are under its influence.
The community room at the base of their building was permanently locked except formal meetings of middle management seemed to happen in there. Several women died alone in their units, former hospital patients with ILLNESSES died of starvation (anorexia), and substances. They were not disabled, they were ill.
Residents, apparently feeling puzzled and vulnerable, asked that the large room be opened for socializing. An intuitive good start. Perhaps that room is monitored by knowledgeable informed personnel that keep tabs rather than simply hosting a social area? Authorities don’t seem to know or find it unnecessary to explain developments.
Perhaps discussion would feel like an admission that the women that died could have received better care and the building better oversight. Though THAT conclusion seems already made. Do authorities understand? Do students, health professionals, patients and their supporters KNOW? Investigations by health professions colleges conclude, No basis in facts appear to support, anything less than adequate, standard, or stellar care was or is in place.
Response you received, “We continue to work with both our tenants and partners to ensure safety and address concerns,” is based on faith. I would have confidence if reflections, goals, and guidelines were listed, available in writing.
LikeLiked by 1 person
I blame the government.
Here in B.C., we used to have many properly staffed, licenced care facilities. Then the Provincial government decided to pass the Assisted Living Act, which allowed for the privatization of care facilities that would no longer require regular supervision to operate.
All political parties were united in agreeing to this fiasco, so all are equally guilty of the disastrous housing shortage that ensued for many poor people — especially the mentally ill & the elderly who require regular, ongoing properly supervised care and other supports to live safely & with dignity in the community.
With few exceptions (excellent housing societies such as Coast Foundation, Mennonite and some other non-profits who still provide good residential care) — properly licenced, supervised housing soon became more and more rare, and more difficult to access.
I am still thoroughly disgusted by the stupidity & cruelty of that bone-head legislative move –and by the ‘good for business’ mentality that resulted in the abandonment of thousands of our most vulnerable citizens.
If anyone wants to see what is called here “the show’,” come to Vancouver & take a stroll by Hastings & Main. It is truly heartbreaking
LikeLiked by 1 person
I was in Vancouver in September and happened to take an Aquabus that serves False Creek. As the conductor was letting off some tourists at Yaletown, he cautioned that what they were about to see may be upsetting. I assumed this might be the closest stop to the Downtown Eastside. The conductor went on the explain that his wife had worked as a nurse in Riverview Psychiatric Hospital where people with mental illness were care for and had programming. He explained that since Riverview had closed many of the former patients could be seen in the Downtown Eastside. Oh, Canada…….
LikeLiked by 2 people
Hi Kathleen thanks for mentioning Riverview. My son was there for about 9 months, before being disastrously discharged 2 weeks before they closed their doors forever. While I don’t think Riverview was perfect in all aspects (it was very far to get to, so visits became an all day affair), but it was very good in other areas. They taught life skills very well, and there were OT workshops and the Penn Hall tuck shop gave patients some social connectcions. The nurses and doctors were excellent.
LikeLiked by 2 people